
")
")
")
TOOTH REPLACEMENTS (CROWNS, BRIDGES AND DENTURES)
For the sake of perspicuity and a better understanding of the tooth replacements available at our clinic, below is a table of contents to facilitate doing searches on, and reading and understanding the treatments detailed in your treatment plan:
permanent, fixed prostheses
Crown
When preparing a crown the dentist grinds down the tooth, takes a precision impression of the tooth stump (prep) based on which the dental technician moulds the master cast and prepares the crown. The crown is intended to restore, strengthen and embellish the tooth. Crowns can be indicated for various reasons:
- if part of the tooth has chipped off or has worn out and can no longer be restored with a filling or inlay in the long term.
- Replacement of an old crown.
- Provision of crowns to root-canal treated teeth.
- If the shape, position and colour of the tooth does not live up to the patient’s demands.
- Implants replacing missing teeth also require crowns.
TYPES OF CROWNS USED IN OUR CLINIC:
All-ceramic crowns (E.Max pressed ceramic)
The substructure of an all-ceramic crown is prepared from pressed ceramic with a novel technology that makes it tooth-coloured, metal-free and lifelike on account of its translucency. Ceramic is fused layer by layer onto the pressed ceramic substructure gradually developing the perfect shape and tooth colour. All-ceramic crowns are chiefly used with front teeth, being as they are the most aesthetic crowns. They are not suitable for long span bridges replacing multiple missing molars as they are not sufficiently solid.
Ceramic veneers (E.Max veneer)
Ceramic veneers are prepared when grinding down too much dentin or tooth enamel is undesired. They usually serve to rectify chipped teeth, discolorations and jammed teeth etc. on otherwise sound teeth. E.Max veneers may also be suitable for fixing crooked gaps. Veneers are prepared by a dental technician and then cemented onto teeth by the dentist
Zirconia crowns
This innovative system combines the solidity of metal-ceramic crowns with the aesthetics of metal-free crowns. Underlying this system is zirconia. Nowadays increasingly, more is heard about the potential effects of metal allergies in dentistry. Accordingly, a new material had to be devised that had the same mechanical properties as dental metal but which triggered no allergic reactions from the human body. With 30 years on the market, Tosoh’s products are completely homogeneous zirconia blocks developed with a sophisticated technology. Since zirconia induces no allergic reactions, it is biocompatible. Its additional good qualities include bad heat conductivity, which ensures that patients will never complain about hot or cold sensitivity. This type of crown is also prepared using the novel computer technology known as CAD/CAM. Additionally, zirconia substructures are tooth-coloured, hence ceramic crowns beautifully blend in with it, and if the gum recedes at the tooth neck in later years, no dark grey lining will be visible.
Materials used for gluing metal-free permanent tooth replacements (crown, bridge, veneer)
Variolink
Variolink is a dual-bonding, light-curing adhesive compound that ensures the bonding of highly aesthetic ceramic and composite restorations. The luting cements form a durable bond between the tooth’s structure and the tooth replacement material significantly contributing to the long-term success of indirect restorations.
Metal-ceramic crowns
Metal-ceramic crowns have a metal substructure onto which ceramic is fused layer by layer. The more layers are fused onto the substructure the more beautiful and lifelike the crown will become. This solution is ideally suited both for single-unit crowns in the lateral area as well as long-span bridges. The metal substructure is strong enough to permanently retain long bridges and since the substructure is fully covered by ceramic, it is aesthetic as well. There is chemical adhesion between the metal substructure and the ceramics burnt thereon, further enhancing stability. One of the greatest downsides of metal-ceramic crowns, on the other hand, is the dark grey colour of the metal
Metal-ceramic crowns have a metal substructure onto which ceramic is fused layer by layer. The more layers are fused onto the substructure the more beautiful and lifelike the crown will become. This solution is ideally suited both for single-unit crowns in the lateral area as well as long-span bridges. The metal substructure is strong enough to permanently retain long bridges and since the substructure is fully covered by ceramic, it is aesthetic as well. There is chemical adhesion between the metal substructure and the ceramics burnt thereon, further enhancing stability. One of the greatest downsides of metal-ceramic crowns, on the other hand, is the dark grey colour of the metal substructure which may lend the tooth a greyish hue at the tooth’s neck, should the gum recede over the years. Furthermore, if the ceramic chips off from the metal substructure due to an accident the crown will be an ungainly sight that can only be resolved by preparing a new crown. Therefore, patients are ill-advised to open beer bottles, to chew chicken bone or wear a piercing with any type of ceramic crowns.
Replacements at our clinic are prepared according to the IPS InLine technology. These are durable teeth conveying a lifelike effect if properly taken care of. The underlying metal substructure is always made of precious metal. It can be prepared from gold, platinum or gold according as we want a warm or a glaring white look. Gold substructures have excellent physical properties since gold has both disinfectant and antibacterial properties. As a result, the crown has an extended lifetime. In former times, this used to be the “high-end” replacement tooth but what with the rise of the price of gold its “competitors” (i.e. Zirconia or E.Max crowns) have pushed this replacement type to the background. The full substructure is encased with tooth-coloured IPS InLine ceramic manufactured by the Liechtenstein-based company Ivoclar Vivadent.
Implant crowns
An implant is in fact an artificial root screwed into the jaw. Once the implant has osseointegrated into the jaw, the new crown can be prepared. An implant suprastructure (abutment) is screwed into the implant using the appropriate torque (35 Ncm) which has a role similar to that of the filed tooth stump (prep), namely, holding the crown in position. This abutment is in fact tucked deep between the implant and the crown. In the mirror, the patient can only see the implant crown or the bridge.
Implant borne crowns can be made of the same material as conventional crowns intended for tooth stumps (preps). The dentists will recommend the material of the implant crown and the suitable solution will jointly be selected with the patient.
In terms of material the following implant crowns exist:
- Max implant crown
- Zirconia implant crown
- Metal-ceramic implant crown
Implant crowns with E.Max pressed ceramic and zirconia substructures are chiefly recommended for the front region based on aesthetic considerations, since in this instance life-like crowns are crucial both as regards colour and as regards transparency. These are metal-free crowns with transparent, tooth-coloured substructures onto which porcelain layers are fused ensuring the best optical properties such as transparency translucency and colour temperature. The most difficult task for a dentist is to replace “just” one crown in the front region as it poses a serious challenge for the dentist to prepare the ideal replacement tooth in the appropriate shape, colour and size. These crowns are prepared according to cutting-edge manufacturing standards (machined from pressed ceramic blocks using CAD/CAM technology) and are obviously in the highest price range. They have the additional benefit that there is little likelihood that a grey metal lining will show around the crown’s collar in later years.
Metal-ceramic implant crowns are the strongest of their kind and highly tolerant of masticatory forces, and hence best suited to replace lateral and posterior teeth. The layered ceramic fusing technique ensures that metal-ceramic implant crowns are aesthetic but due to their dark metal substructure, different optical properties may prevail as compared to metal-free crowns. In this group of crowns too, metal-ceramic crowns are the most reasonably priced ones and a good dental technician is sure to achieve outstanding aesthetic results.
In terms of the type of retention, there exist 2 kinds of implant crowns:
- cement-retained implant crowns
- screw-retained implant crowns
Cement-retained implant crowns are glued onto the abutment using provisional or permanent luting cement. It is immensely important that a thread (gingival retraction cord) is placed between the gum and the abutment in order to enlarge the gingival sulcus since cement spilling over may remain under the gum once cured. This is particularly dangerous if the implant is placed deep under the gum since there remains a non-cleanable surface to which microorganisms may adhere causing inflammation and infection or the incidental rejection of the implant. However, with a gingival retraction cord placed inside in anaesthesia, all surplus adhesive can be removed with ease. Cement-retained implant crowns are way more aesthetic than screw-retained crowns, as their top is not bored through, which allows the dental technician to design a tooth-coloured masticatory surface in line with the rest of the crown. They are furthermore less expensive than screw-retained crowns, which require a more expensive abutment. That said, they have the major downside that once the crown gets damaged due to an accident or the implant gets inflamed (peri-implantitis develops) which necessitates treatment, the only way to access the area to be treated is by cutting off the crown which needs to be prepared anew.
The major benefit of screw-retained crowns is that whatever happens, e. g. the ceramic chips off from the crown or an inflammation (peri-implantitis) develops, the crown can be screwed off, the inflamed implant can be treated and the crown rectified, in other words, interventions are a great deal easier. On the other hand, screw-retained crowns are costlier to prepare than cement-retained crowns and they fall behind in terms of aesthetics. Due to the different axial inclination of the implant, the bore of the screw retaining the abutment and the crown opens onto the surface of the tooth. Although once abutment is screwed in, the dentist prepares a matching aesthetic, tooth-coloured filling on top of the crown, but that will not be on a par with that fused from ceramic by the dental technician. For future comfort, certain compromises need to be made as to aesthetics.
Implant crowns made with CAD/CAM technology represent also state-of-the-art accuracy. The dental technician using conventional multi-layer ceramic veneering does not mould this type of crown, but the tooth’s shape, colour, etc. are designed with a computer and the crown is milled by “lathe” from a block of pressed ceramic or zirconia.
Bridge
Bridgework is fixed tooth restoration that consists of several crowns linked together. The bridge replaces one or more missing teeth filling up the gap between two adjacent teeth. When preparing a bridge the adjacent teeth requiring filing and a precision impression needs to be taken of the filed teeth (prep) and the dental technician prepares the bridge the same way as the crowns. Bridgework is no longer the preferred method of tooth restoration, as it often requires completely sound teeth to be grind down. Patients therefore tend to opt for tooth implantation. The main advantages of a tooth-borne bridge are its affordability and short lead-time as opposed to implant borne bridges, which are more expensive and require several months’ healing time.
Bridges are made using the same technology and materials as crowns, so you may also want to read the section describing crowns.
As regards their material, the following bridges are available:
E.Max pressed ceramic bridges
E.Max pressed ceramic bridges are used in the area of anterior teeth or the replacement of lateral teeth. In terms of aesthetics, this is considered the cutting edge method.
Zirconia bridges
This is a heavy-duty bridge highly tolerant of masticatory forces making it suitable for replacing several missing posterior teeth. E.Max and zirconia bridges yield better results as regards aesthetics but are more expensive than metal-ceramic bridges.
Metal-ceramic bridges
Metal-ceramic bridges are the most resilient and durable tooth replacements, excellently suited for the replacement of posterior and lateral teeth and even convenient for the replacement of long-span edentulous areas. It is best bridge type in terms price. However, it has the drawback that if the gum recedes from the dental cervix in later years the edge of the bridge may sport a greyish hue, which can be particularly disconcerting if the patient has a high smile line.
Implant-retained bridge
Implant-retained bridges are tooth replacements supported by implant bars inserted into the jaw, that is, the pillar of the bridge is not a filed tooth stump (prep) but an implant.
As regards their material, the same types of fixed implant bridges are available as detailed in the section on implant crowns.
- Max pressed ceramic implant bridge.
- Zirconia implant bridge.
- Metal-ceramic implant bridge.
To sum up, metal-free implant bridges such as E.Max and zirconia are more aesthetic and more expensive and are chiefly used for front teeth. Metal-ceramic circular bridges are designed for heavy-duty use and can be attached to anything between 2 implants to 8 implants.
As regards their retention, implant bridges are manufactured with the same technique as implant crowns and display the same advantages and disadvantages.
Materials used for gluing metal-free permanent tooth replacements (crown, bridge, veneer)
Variolink
Variolink is a dual-bonding, light-curing adhesive compound that ensures the bonding of highly aesthetic ceramic and composite restorations. The luting cements form a durable bond between the tooth’s structure and the tooth replacement material significantly contributing to the long-term success of indirect restorations.








DIGITAL DENTISTRY
Fast, accurate and indispensable. With the new era of digital dentistry beckoning, we now have the Wireless Medit i700 intraoral scanner at your service.
The lifelike digital likeness of the dental arch or tooth preparation is immediately displayed in colour on the screen to be viewed in 3D by the patient and their dentist. The greatest benefit of digital technology is the reduced lead time required for the fabrication of replacement teeth and crowns, owing to the maximal precision of planning, seeing as no courier is involved in the process and no master cast is required for the tooth preparations: the digital impression is on the dental technician’s computer at the click of a button.
REPLACEMENT TEETH FABRICATED BY MEANS OF DIGITAL IMPRESSIONS
With the use of an intraoral scanner the following fixed tooth replacements can be prepared: inlay, onlay, crown, bridge, implant-borne crown. Replacement teeth fabricated with the help of digital impressions are a lot more accurate than those prepared using conventional (analog) impression taking methods. Following impression taking the dentist can assess their work from multiple perspectives and with 100% accuracy, unlike in the case of impressions taken through well-established, conventional means. In this fashion, shortfalls that would normally go unnoticed for days later until the dental technician detects them, are evinced immediately. Faults are indicated by the computer thus the dentist’s work can be rectified in the dental chair itself.
Many people are intimidated by having their replacement teeth prepared or replaced due to the nausea experienced during impression taking. In the course of digital impression taking, however, patients no longer have to reckon with such discomfort seeing as the scanner is equipped with a small sized head. As opposed to the conventional method, no big copings and impression material is introduced into the patient’s mouth, but an oral scanner the size of a small tooth brush takes photographs of the teeth, tooth preparations as well as occlusion.
Digital dentistry has brought about an incredible breakthrough in the field of implant-borne implants and bridges. With the help of a Scanbody, digital impressions can be taken of the implant and the surrounding gums, thus the prospective replacement tooth can be accurately secured both onto the implant and the surrounding soft tissues.Also, a great advantage of digital dentistry is the fact that it is perfectly suited for the circumvention of allergic reactions liable to arise in conventional dentistry with patients allergic to impression materials.


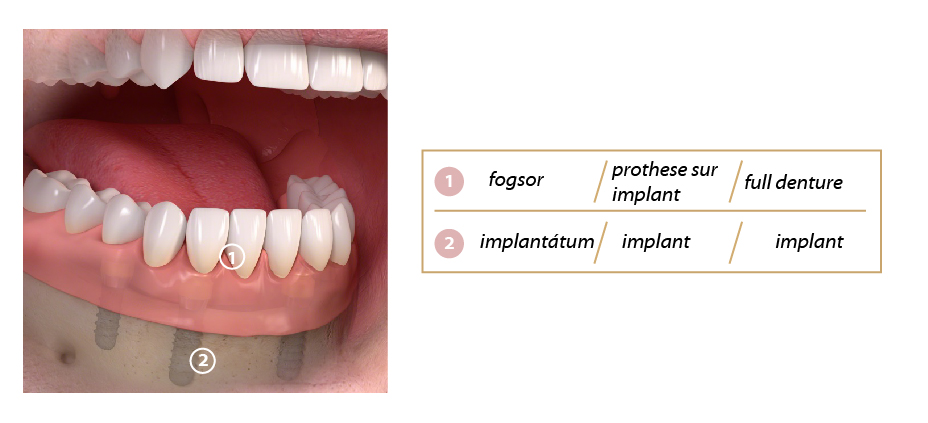
Permanent removable dentures
Steps of preparing removable dentures intended for implants
Three dimensional X-rays (CT) in DICOM in ICat format.
During a personal consultation the dentist examines the oral cavity and to map the anatomic relations of the jawbone using CT.
The dentist draws up the treatment plan.
Surgical phase: the implants are installed.
A 3 to 6 months’ healing time ensues during which the implants osseointegrate (integrate into the bone).
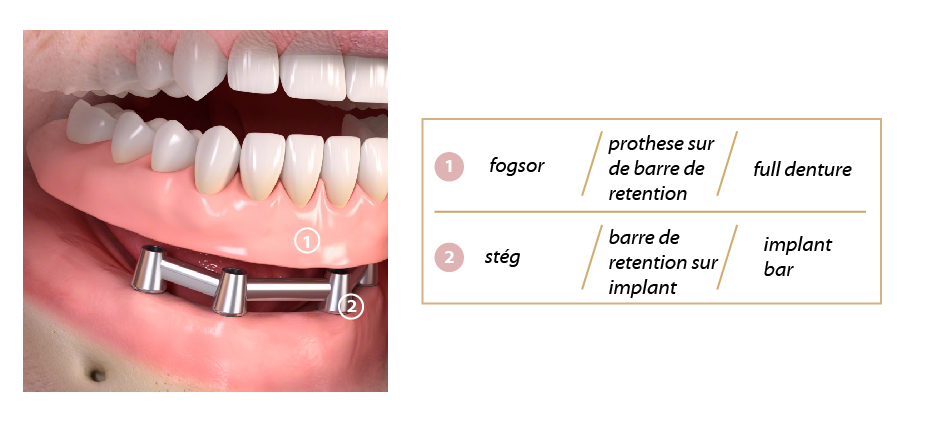
Prosthetic phase: once healed, the dentist takes impressions of the implants integrated into the jaw. Gnathology and bite registration serve to determine the patient’s bite and the aesthetics of the teeth. The bar and denture are then prepared by the dental technician in a laboratory. The dentist fixes the abutments, viz. bars or Locator systems, as the case may be, on the implants, to which the overdenture (i. e. a removable denture ) is attached. Check-ups and minor bite corrections are indispensible every few days as the patient’s muscles and the jaw joint (temporomandibular joint, or TMJ, for short) require time to adjust to the new tooth replacement before everything comes into alignment. Such check-ups are worth the trouble and time as an inappropriately adjusted bite may overload the denture and the implants. Undue pressure is particularly dangerous for implants as it may bring about bone resorption and cause the implant to come off and the teeth to break off from the denture.



Permanent, removable dentures
Provisional crowns or bridges prepared by the Scutan method
With fixed replacements (crowns or bridges) the tooth is drilled and prepared for a precision impression on the first day based on which the dental technician prepares the permanent crown or bridge. Depending on the number of crowns, the permanent crowns are prepared in 5 to 10 days. For this period, an immediate chairside provisional crown or bridge is prepared on the spot (direct provisional crown). No patient leaves the clinic without teeth. Benefits associated with provisional crowns are as follows:
- protects the prep against the so-called dentin wound developing in the course of filing which is extremely sensitive to cold, warm and other chemical stimuli. Freshly filed live teeth are like our hands without skin following an accident: they are oversensitive to everything; even something as ordinary as breathing may cause pain.
- It holds the prepared tooth stumps in position preventing them from migration caused by masticatory forces until such time as the crowns or bridges are prepared. If the tooth stump migrates the tooth replacement will not fit in, only if pressed hard or pried… and when forcing it into position the bridge may come under undue strain, the ceramic may disengage from the substructure, and the preparation of the crown and ceramic coping may start all over again much to the delight of all and sundry – including the patient, dentist and dental technician.
- Aesthetic corrections or trial dentures can easily be made from this material, allowing patients to avail themselves of a simple, quick and inexpensive trial fitting with the help of which they can easily imagine their prospective tooth replacement.
- Chipped off teeth, metal posts etc. can easily be covered with a provisional crown.
- It is quick and inexpensive to repair.
Due to its drawbacks patients are not advised to leave the vicinity of the dental clinic, as:
- its material is of inferior quality as compared to that of the crown prepared by the dental technician, wearing time should therefore not exceed 2 to 3 weeks, by which time the permanent ceramic tooth replacement is prepared.
- It is less aesthetic than a provisional crown prepared in the laboratory.
- It is more susceptible to breakage.
- It is likelier to get discoloured.
- It is glued on with a weaker adhesive so that the dentist can easily remove it a week later, similarly, it is likelier to come off the tooth preparation and may have to be glued back on several times.
Long-term provisional crown or bridge made using the PMMA method
Long-term provisional crowns or bridges are prepared by the dental technician (indirect provisional crown). The dentist prepares the teeth and takes a precision impression thereof and the dental technician prepares the long-term provisional crown in 3 to 5 days. Such fixed temporary replacements are indicated in the following instances:
- with neglected periodontal diseases it often occurs that the infected gum bleeds to such an extent that no proper impression can be taken of the tooth preparations. In this case a pre-prosthetic treatment is in order (scaling, open or closed curettage, etc.) to eliminate the infection around the dental cervix. Healing may take up to 6 months, and flawless impressions for the permanent replacements can only be taken once the wounds have completely healed.
- Many chipped or carious teeth require root canal treatment and a post and core procedure in several sittings, in other words, 2 or 3 hours’ dental treatment will not do. In such cases the teeth are filed and a long-term provisional bridge is prepared that can be removed each time the teeth underneath undergo several days’ treatment.
- If occlusion is out of alignment, the patient has an incorrect bite (malocclusion) and a gnathological treatment or bite correction is indicated, a long-term provisional bridge is prepared for 6 months and we examine if the new bite with the new teeth is comfortable. The permanent replacement is only prepared once improvement is observed.
- Beautiful test and diagnostic crowns can be prepared for the patient to see what kind of teeth (colour and shape, length, etc.) they are going to have. The patient goes home with the beautiful new long-term provisional crowns and may jointly decide with their family if the new crowns live up to their expectations. On returning for the permanent replacement, the patient will have definite ideas as to what kind of teeth they desire compared to this provisional one. If the patient was content with the provisional crown, a photograph and an impression will be taken of it which will be used and duplicated as reference material by the dental technician in preparing the permanent crowns.
Disadvantages associated with long-term provisional crowns:
- it is more expensive than provisional crowns prepared by the dentist since it is made from a more durable, resistant and resilient material.
- It takes several days to prepare.
- It is glued on with a stronger luting cement, so when the patient returns to continue their treatment several weeks or months later it can only be removed by cutting off, in other words, a new one is required for the relevant week of treatment.
TEMPORARY REMOVABLE DEFLEX DENTURES
The temporary removable denture, Deflex denture, is made of flexible nylon denture material, which is used as an immediate denture after tooth extractions and implantation, so that the patient is not without teeth for a day.
The material is manufactured by NUXEN SRL in Buenos Aires and contains no monomers or metals, so it does not cause any irritation or allergies.
Thanks to its elasticity, the chewing pressure is distributed, causing less cracking than with hard dentures. It is impact resistant and does not break under normal conditions. Translucent, aesthetic, light, thin, does not interfere with the patient's speech.
Acrylic is particularly recommended for sensitive and nauseous patients, is easy to get used to, and is very popular with users.
The material is manufactured by NUXEN SRL in Buenos Aires and contains no monomers or metals, so it does not cause any irritation or allergies.
Thanks to its elasticity, the chewing pressure is distributed, causing less cracking than with hard dentures. It is impact resistant and does not break under normal conditions. Translucent, aesthetic, light, thin, does not interfere with the patient's speech.
Acrylic is particularly recommended for sensitive and nauseous patients, is easy to get used to, and is very popular with users.
Adhesives used for cementing provisional tooth replacements (crowns, bridges)
GC Fuji TEMP LongTerme
Crowns and bridges are not always glued on permanently. They are often glued on provisionally due to certain inflammations, pains or merely for the sake of testing. GC Fuji TEMP LT ensures a long term, secure temporary retention, and easy removal of bridges and crowns as necessary after a few weeks or months. It is easy to use, yet reliable.
Manufactured by GC, típusa Fuji Temp LT, Japan

Gnathology – the importance of correct bite registration
Gnathology translates as the study of bite or chew and this science deals with correct occlusion (bite and chew).
It is not only important that our teeth and replacement teeth are well-maintained. They should also ensure correct, efficient and comfortable chewing.
Gnathology is a science dealing with the anatomy and operation of teeth and other elements participating in the act of biting such as the mandibles, masticatory muscles, temporo-mandibular joints, etc. For producing accurate and high-quality, replacement teeth (crowns, bridges, dentures) state-of-the-art and high-precision diagnostic devices and methods are used such as customised articulators, face-bows, supporting pin registration. For a perfect prosthodontics job not only is the accuracy and beauty of the replacement teeth important, equally important is the accurate registration of the maxilla-mandibular relationships, the position of the jaw joints and the anatomical properties of the jawbones. Simply put, it will not suffice to have a beautiful car, the wheels, the crankshaft, etc. all need to be well adjusted for a smooth drive.
Customised articulators, face-bows, supporting pin registration fulfil the following roles:
- the determination of the ideal, “rearmost” or “middlemost” position of the temporomandibular joints.
- The determination of the centric relationship with Gothic arch tracing.
- Registration of the axis of the condyle trajectory (relative to the skull).
- The determination of occlusal height.
- The registration of the correct anatomical and functional characteristics of the temporomandibular joints.
- The exchange of the occlusal data measured and registered between the dentist and the dental technician.
Devices used for gnathological treatment, the determination of occlusal data and bite registration
AMANNGIRRBACH ARTEX System
AMANN GIRRBACH ARTEX System is a comprehensive and customizable articulator by means of which the occlusal data and the ideal position of the temporomandibular joint can promptly and accurately be registered and forwarded from the dental clinic to the dental laboratory.
Designed for daily use, it is made from strong steel based on 25 years’ experience and recognised the world over for its durability.
Manufactured by Amann Girrbach, Austria.
Artex facebow
With the help of a face-bow, all essential anatomic information necessary for the preparation of a perfect tooth replacement can be collected in a matter of minutes. The face-bow can accurately capture the axial position of the maxilla (upper jaw) relative to the skull.
The face-bow opens in a symmetrical fashion ensuring that the midline can be precisely registered. Due to its ease and quickness of use, the patient experiences no discomfort at all.



